This brief is 100% free to read. No login required.
Evidence verified against 2024-2025 systematic reviews
Beyond Medication: A PT's Guide to Cognitive Rehabilitation for MS
Cognitive impairment is a common and frustrating symptom for people with Multiple Sclerosis. This brief provides a practical guide to evidence-based cognitive rehabilitation strategies that you can implement to help your patients improve memory, attention, and daily function.
Research: January 2026
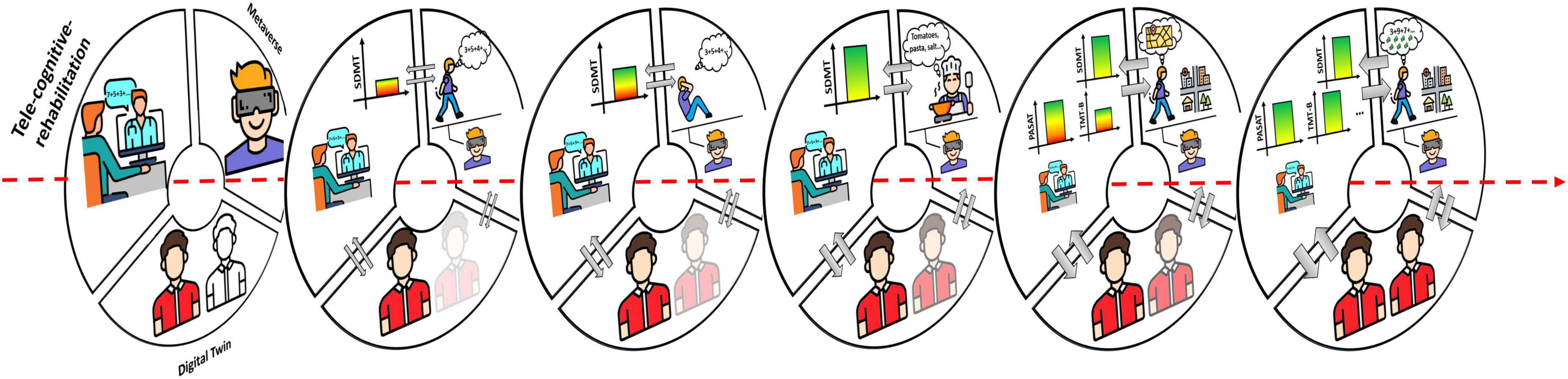
This diagram illustrates the mechanisms of cognitive impairment in MS and the pathways through which neurocognitive rehabilitation can intervene.
Related Videos
Cognitive Rehabilitation for Patients with Multiple Sclerosis
Ask an MS Expert: Cognitive Rehabilitation in MS
Key Findings
- 1Cognitive rehabilitation is an effective, low-risk treatment for MS-related cognitive impairment.
- 2Both restorative and compensatory strategies have been shown to be beneficial.
- 3Digital health platforms and tele-rehabilitation are making cognitive rehabilitation more accessible.
- 4Consistent, tailored cognitive training can lead to meaningful improvements in daily function.
Clinician's Note
What I've found works best is to integrate cognitive tasks into our physical therapy sessions. For example, while your patient is on a stationary bike, have them do a verbal fluency task, like naming as many animals as they can in a minute. This dual-tasking approach mirrors the real-world cognitive demands they face. It also helps to frame it not as 'fixing' their brain, but as 'training' it to be more efficient. Empowerment is key. When patients see they can take control of this aspect of their MS, it's a huge psychological boost.
Clinic Action Plan
Common Mistakes to Avoid
- •Using generic brain games instead of evidence-based cognitive rehabilitation programs.
- •Not tailoring the intervention to the patient's specific cognitive deficits.
- •Failing to integrate cognitive tasks with functional, real-world activities.
- •Neglecting to monitor for fatigue and adjust the program accordingly.
Frequently Asked Questions
This brief includes an extended deep-dive section with clinical nuance, dosing details, edge cases, and special population considerations.
Unlock with Premium — $99/yrWant more from NeuroDash?
Save protocols, track CEU hours, download PDFs, and get unlimited AI access.
Explore Premium — $99/yrMore in MS
HIIT for MS: A Practical Guide to Improving Fatigue and Exercise Capacity
This brief provides a practical, evidence-based guide to implementing High-Intensity Interval Training (HIIT) for patients with Multiple Sclerosis. It covers the why, the how, and the what-to-watch-out-for, so you can confidently prescribe this powerful intervention to improve patient outcomes.
A Practical Guide to Fall Prevention in Multiple Sclerosis
Falls are a serious and frequent problem for people with Multiple Sclerosis, but they are not inevitable. This brief provides practical, evidence-based strategies you can use to significantly reduce fall risk in your patients with MS, focusing on targeted exercise and functional training.
Mastering Gait in MS: A Practical Guide to Task-Oriented Rehab
This brief breaks down how to use task-oriented training to improve walking in your patients with MS. It’s a practical, evidence-based guide to move beyond generic exercises and create targeted interventions that get real results.
Beyond Baclofen: Modern Spasticity Management in MS
This brief outlines practical, evidence-based strategies for managing spasticity in your MS patients. It moves beyond just medication, focusing on targeted physiotherapy and what the latest research says about what really works.